No products found
Search in progress...
Filter by:
Type Family Sub Family
Filters
Products found:

Before describing its content, we want to illustrate the purpose and importance of the project “Spine Leg Toolkit”. The examination of the locomotor system concerns many professional figures, the orthopedist, physiotherapist, physiatrist, orthopedic technician, pediatrician, sports doctor, motor sciences doctors, just to mention the main ones: every professional has his own goals and objectives strategies but also many shared points.
In particular, evaluating the alignment of the spine and lower limbs means first knowing the variability of the various parameters present in the population, age-related changes and finally the thresholds beyond which we can speak of anomalies or pathology. The mere observation is no longer sufficient: it gives us a first impression, qualitative data, too vague limits. Especially if we want to check a normal threshold, the trend over time or document the effectiveness of our therapeutic measures, we have absolute need for numbers, precise data. On the other hand, the daily use, in the surgery or in the gym, requires simple data, not bulky and above all non-invasive tools.
For this reason the “Spine Leg Toolkit” case has been designed, as an accurate choice of clinically tested tools to evaluate a high number of clinical interest parameters: frontal and sagittal compensation of the head and trunk, rotations on the transverse plane in static and in flexion, the sagittal curves, the heterometry of the lower limbs, the alignment and the foot length, together with joint angle measurement and analog scale ache. For the first time the professionist finds what he needs all inside a single case, which, we are sure, will become an essential accessory.



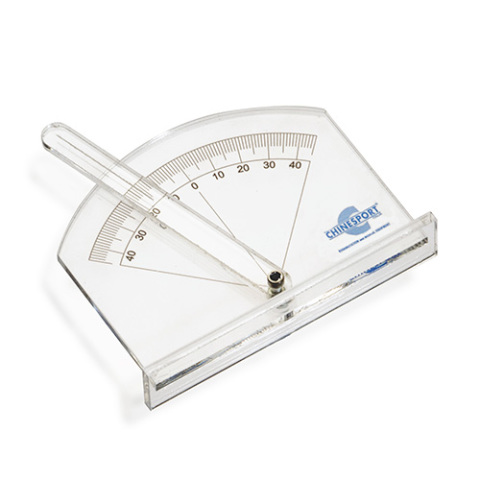
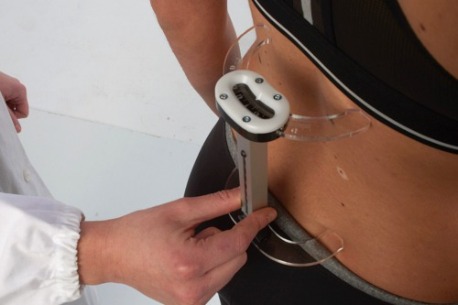
A simple measuring tool for the hump (trunk rotation angle) and for the Cobb corner
In patient measurement - standard position with patient on extended knees, flexed trunk, arms abandoned in front, the tool is placed gently on the back, the rod comes then rotated until it is “leveled”; the degree of inclination can be read immediately or even, unlike other tools, removing the instrument from the back and keeping the rod between the thumb and forefinger, thus allowing an even more precise reading. Scrolling along the back, from the thoracic to the lumbar tract, you can identify the most rotated section (s) and record its level.
In radiographs measuring the edge of the instrument comes next to the edge of the vertebra upper limit of the curve, the rod is then rotated until it is “leveled”; the degree of inclination is read on the protractor scale; the operation is then repeated for the lower limit vertebra. Cobb’s angle is given by the sum of the angles of inclination of the two limit vertebrae. The inclinometer is also useful for the precise identification of the limit vertebrae, which are the most inclined.



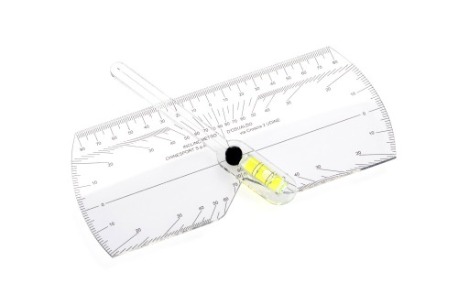
A precise tool for non-invasive measurement of kyphosis and lordosis
The principle behind the tool is the axiom that for three points only one circumference passes. The tool provides us with two data related to the tract of measured spine, approximated to an arc of circumference: the arrow and the rope. Starting from these two data we can obtain: the radius of curvature and the subtended angle, corresponding to the Cobb angle evaluated on the radiography.
The arcometer is a particularly useful tool as an integration to the clinical examination, screening for specialists, follow-up of the patient with curved back already radiographically evaluated: even if it does not replace radiographs, it helps to reduce their numbers. It also allows you to evaluate the subject both in spontaneous and self-correcting position, useful element for assessing the stiffness of the curve, for a judgment on the course and to evaluate the effectiveness of the kinesitherapy and / or orthotic treatment. The instrument is also equipped with a central rod with smaller diameter foot to allow the evaluation of the corset correction (by providing the dorsal pelota with a special hole).
To facilitate the calculation
To measure kyphosis or lordosis, the arcometer is positioned with the side rods at the end of the curve. That value represents the rope. The central rod is brought to the medium point of this distance and therefore is approached to the back; her millimeter scale gives us the value of the arrow. The value of the Cobb angle and the radius one are obtained by a simple chart with two entrances which is supplied together with the tool.



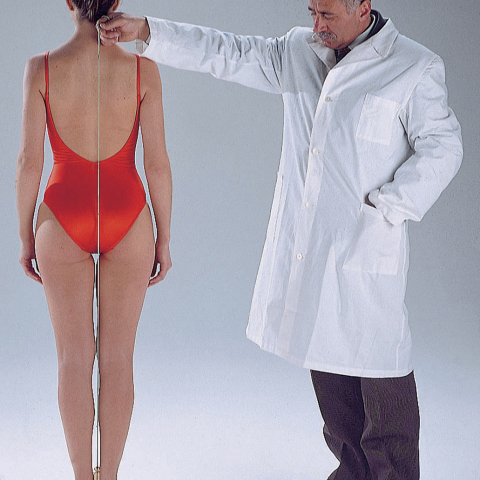
A revisited tool for asymmetries measurement
If we only think of a case of lumbar scoliosis and try to describe the hips asymmetry in a report, we find ourselves in using more or less vague terms such as “moderate, evident, remarkable”, certainly not wrong but of little use for comparison.
In the context of a visit for the spine the caliber allows us to quantify the alignment asymmetries on the frontal plane and in particular to evaluate the movement of the head, of the upper trunk part or hips, with respect to the midline, taking for this purpose the inter-gluteal line or alternatively the bisector of the base.
A lateral shift of the midline of the head it’s described by the term decompensation, a shift of the median line of the shoulders or hips is described as front, right or left translation respectively. This shift can be indicated in absolute values (cm) or better in percentage (% of translation) suggestable modality in progress for anthropometric changes affecting the trunk.
To facilitate the calculation
To facilitate the calculation of the translation percentage it’s available a simple two-entry chart along with the instrument. This tells us with a single number how much, in percentage, the center of the measured segment is displaced laterally than the theoretical center of symmetry. The formula used is the following: a-b / a + b%, where as numerator appears hence the difference of the two segments defined on the instrument by plumb line, as denominator the sum of the same segments.


A practical tool for measuring the trunk rotation in orthostatism
The evaluation of a subject with suspected scoliosis using a torque meter is carried out in a standing position. The basis of the tool is put to the sacrum; in this way a zero plane is defined as reference, with respect to which the alignment of the trunk on the transverse plane to the desired level will be read: from lumbar to middle back.
When the mobile element is placed against the back, it will slide into its housing by a corresponding number of degrees to the rotation of the trunk. An index on the housing indicates with precision degrees of rotation.
The tool is suitable for a diversified use:



An adaptive lever, still useful today
The bubble placed in the center of the main bar tells us essentially if the pelvis is levelled, when patient is positioned in orthostatism with load well distributed on the two lower limbs. Otherwise the operator will place one or more raises on the falling side, until the instrument will be levelled. At this point it will be possible to check the pelvis alignement and quantify the difference in length of the lower limbs. For this purpose, the raises kit 06730 can be useful.
Note that the evaluation of a difference in length of the lower limbs requires a lot of attention. Indeed mistakes are possible either for incorrect positioning of the subject but also for presence of anatomical variables, such as asymmetric skeletal pelvis, twisting of the lower limbs, laxity of one or more joints, musculotendinous retractions. To improve the evaluation accuracy it is therefore suggestable to use multiple measurements in different postures, now made possible by the different tools contained in this kit.


For measuring the length (heterometry) difference of the lower limbs
To measure, the patient is positioned supine and well aligned: head aligned with zenith nose, trunk aligned, lower limbs parallel with zenith positioned kneecaps. The operator therefore makes sure that the instrument has the longitudinal axis well aligned with the legs. Then he proceeds by placing the fixed platform next to the left foot, exerting moderate pressure to ensure good adhesion to the whole plant, and in particular to the heel. He approaches then the right, mobile platform, exerting equal pressure. The difference, on the millimeter scale, can be read at this point, or after removing the instrument (taking care not to alter the relation between the platforms). In case of retraction of the Achilles tendon we will only be able to measure functional heterometry.



A simple tool for objective hindfoot axis evaluation
To collect measurement, the instrument is brought close to the hindfoot, with the examinated patient in static position, preferably on a plane raised above the floor to facilitate the reading. The pointer is oriented parallel to the hindfoot axis and the value of valgus or of varism is immediately readable in degrees.
Normality limits cannot be indicated absolutely, since they may vary according to age and loading methods (mono or bipodalic) and the scientific literature itself provides heterogeneous values. However in the child it can be roughly indicated as a threshold of attention, a valgus superior than 8-10 °, any varism value and significant asymmetries between the two sides.
In doubtful cases it is not much the absolute value but rather the trend over time that can guide us for a physiological or pathological situation. For this purpose the tool, for its ease of use, is particularly useful by allowing repeated measurements at longer or shorter intervals. This is particularly valid in the young child, where the laxity of the ligamentous structures frequently involves major deviations in valgus of the hindfoot, while loaded , however usually progressive improvement are noticed with growth. Even the difference in value of the hindfoot angle in monopodalic load compared to the bipodalic one, could provide clinicians with important information.


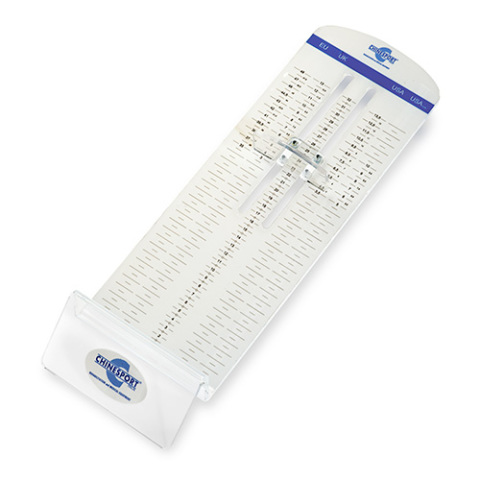
An ancient tool for collecting new information
On a first visit, often information on growth foot is not available and in this case we can enhance the foot / height comparison. In fact, a high comparison, over 16, 16.5%, will indicate a phase of acceleration of the foot and therefore one initial pubertal development. A low comparison, less than 15% in one teenager with secondary sexual characteristics, already mature, will tell that we are in a phase where the height growth is slowing down.
It should certainly be taken into account the variability present in the population: there are small people with long feet and vice versa, however for the clinician who has to take important decisions, also the foot growth speed value and the comparison between foot & height, have an important value, near all other anamnestic data and secondary sexual characteristics, equally variable.


A classic, always essential tool
Pain assessment is recognized today as an obligation for each user who is taken in charge and its documentation represents an essential standard for every healthcare facility. The instrument presented here has a double scale: the method of smileys (Wong Baker) for the child from 3 years and the VAS scale (visual-analogue scale) from 8 years onwards. In the first one, the choice is made from a series of smiley faces with different expressions, in the second a cursor indicates the score along a graduated scale from 1 to 10. The pain scale usually depends on the user and, subsequently, at shorter or longer intervals depending on the problem, acute or chronic.

GPS Postural labs - Introduction - Modularity - Main parts - System requirements - Complementary services - The different models - GPS software - Static posture assessment - Stabilometric analysis - GPS Postural Labs technical data - Podoscope models - Podoscopes - Podoscopes with GPS software - D’Osualdo set - For analysis of the back - For analysis of lower limbs - For postural assessments - Scales and x-ray viewers - GPS ACADEMY - Education program - GPS Therapeutic Pathways
Brochure, Ed. April 2024, English. 60 pages.