
No products found
Search in progress...
Filter by:
Type Family Sub Family
Filters
Products found:


Among the mechanical causes we can include radicular syndromes due to protruded or herniated discs as well as the insidious spinal stenosis syndromes, in which lumbo-sciatic pain is associated with forms of claudication resembling those caused by vascular pathologies. Patients formerly submitted to surgery and now suffering from its consequences, or relapses of previos syndromes are also elegible for treatment. The most interesting field of application of this method mainly concerns cases for which all previous treatments have proved ineffectual or when pain has persisted for at least 4 weeks.

Initial positioning of the patient
The patient is invited to take off his/her shoes, trousers or skirt. It is not necessary to take off all clothes unless they prevent the patient from moving his/her upper limbs freely. While the patient is still standing, a pelvic belt will be put on him Although not fastened. After these preliminaries, the patient is required to lie supine on the treatment table, as shown in Figure 1.
The terapist checks if pain increases when the patient stretches out his/her lower limbs. If so, tratment will continue as indicated in Figure 2. If pain does not increase, the patient will remain supine and stretch his/her lower limbs. The lumbar region should be positioned over the opening between the two sections of the table; the patient’s positioning down not require centimetric precision.
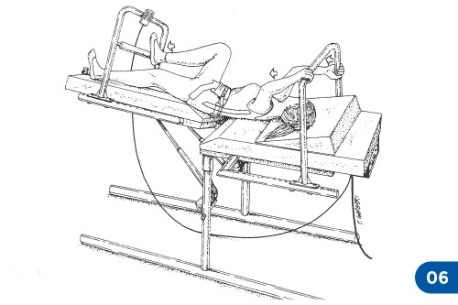
The terapist will then start to tilt, extend and rotate the table distal section in both directions so as to determine which positions cause a possible increase or else a decrease in pain. At this stage, the patient might be requested to lie on his/her side (Figure 4). In this case, the flexion/extension of the distal section of the table will induce a right or left inclination of the patient’s lumbosacral spine.
Treatment will start with the patient lying in the least painful position, in any. Otherwise, the treatment will be administered with the patient lying in a supine position.


Patient’s “anchoring” to the treatment table
At this point the pelvic belt must be fastened and hooked by means of special strap to the fixing ring placed in the legs section of the table. The strap should not be very tight. This procedure is not aimed at producing a passive pelvic traction, as in the conventional traction treatments. Rather it is meant to prevent the patient from slipping towards the head section of the table while he is doing strong active traction exercises with contemporary lower limb pushing. If the patient is eccessively overweight or lacks muscular strenght, body friction against the table will already be enough to keep him steady.When the use of a pelvic belt is not advisable, the patient can maintain a steady position by “anchoring” his feet to the bars of the treatment table (picture 3).
Upper limbs and head positioning
In general the patient’s hands should be placed at half lenght on the vertical bars. If the patient cannot easily abduct one or both shoulders, he/she can keep his/her arms abducted and hold onto the horizontal bar located over his head. A wedge cushion can be put under the patient back so as to keep his/her trunk and head slightly flexed.
Active Lumbar Traction: the manoeuvre
Let’s suppose that treatment is performed, as it usually happens, with the patient being lying on his/her back. Figures 2 and 3 show some standard TLA movement patterns. The patient simply “pulls himself/herself” with his/her arms exerting maximal effort for 5-6 seconds and then relaxes. Both traction and relaxing have to be gradually developed. As a general rule, patients are expected to do this exercise holding their breath (“hold your breath while you are pulling yourself”). After that, there is a rest of 10-60 seconds.


Although it may seem very simple, this exercise is not always properly performed. The most common mistakes are the following:
All of these mistakes can easily recognized
In order to prevent back arching, it might be useful to ask the patient to flex his/her lower limbs and place his/hr feet on one of the table rear bars. Sometimes the therapist can ask the patient to assume the initial position as shown in Figure 3. After the therapist has placed one hand under the patient’s heel or buttock, the latter is expected not to press onto the therapist’s hand while pulling. [...]
For more information and details we invite you to see the Active Lumbar Traction handbook for treatment guide lines, clinical and pathophysiologic review.
“The Active Lumbar Traction, or TLA, originates from the Swedish method of “auto-traction”, a mechanical type of treatment for lumbosciatic pain. This manual is divided into three chapters, each one independent from the others. Readers who wish to have a preliminary idea on the method should look directly at the third chapter, where the subject has been concentrated in 15 questions with relative answers. If, on the other hand, readers are already acquainted with the general principles of the method but wish to understand it's practical use, they can refer to the second chapter, which deals with the treatment technical procedures.
Readers willing to know about the origin of the method and its scientific premises should instead go through this introduction and the first section of the manual. Anyway, after reading those two sections they can decide whether to skip the rest if not interested in the method.”


The active Lumbar Traction is a method consisting in therapeutic rehabilitation exercises and as such it must be prescribed by a physician and administered by a therapist.
The treatment can be applied to a wide range of conditions defined in various ways: back pain, sciatica, narrow canal syndromes, herniated disc, radiculitis and so on. “Lumbago” and “sciatica” are insidious clinical conditions. Most of these syndromes are ultimately caused by a benign mechanical compression on the nerve endings due to disc herniation or protrusion. The latter might occur with or without the existence of bone dysmorphologies (osteophytes, congenitally narrow canal) and with the interference of the above-described vascular processes.
A small part of the above described syndromes are on the contrary due to an incredibly wide range of pathologies, such as, for example, aortic aneurysm, vertebral metastasis, osteoid osteoma, spondylolisthesis and many others. Fortunately, our treatment turned out to be harmless for most of these cases; however this is not a good reason to administer it uselessly.
Very often our typical patients volunteer for ALT treatment after a long diagnostic and therapeutic history. Patients might not have been already submitted to examinations, such as rays, CT or NMR. In this case, if we presume that the patients’ symptoms are caused by a disc protrusion or by a narrow canal syndrome (and surgical intervention does not seem inevitable) it is reasonable to start with 3 sessions of Active Lumbar Tractions. Further examinations shall be made only if the treatment proves ineffective.
The general and logical clinical pattern very seldom indicates that the ALT treatment is not recommendable. Sometimes it might be better not to use a pelvic belt. In alternative, the patient will have to use the dorsum of his/her feet for “self-anchoring” on the treatment table, as we will explain later on. The doctor must keep in mind that the active traction effort requires an intense Valsalva manoeuvre as well as a considerable paravertebral muscle activity. This must be considered before prescribing the treatment. Consequently, there is no sense in establishing fixed parameters in order to determine whether elderly patients or patients affected by cardiopathologies, osteoporosis, inguinal hernia or any other concurrent syndromes can be eligible for therapy. The final decision depends on the doctor who, of course, will have to rely on the experience of the therapist whom the patient is entrusted to. According to our experience, the most frequent contra-indication are the existence of inguinal or crural herniations (also already surgically treated) and of cervical or shoulder pain.
In the first case it is absolutely advisable to avoid using a pelvic belt, where a hernial strap might be advisable. Patients should be instructed not to exert maximum efforts, even to the cost of prolonging the treatment cycle. With the second type of patients, positioning and intensity of traction manoeuvres must be individualised according to each single case so as to minimize the pain deriving from the upper limb efforts. Anyway, an increase in lumbar and cervical pain after one session does not compromise the treatment chances of final success. Sometimes, it only means that therapy should be prolonged.
In theory, active traction efforts without the use of a pelvic belt are harmless also if applied to pregnant women, at least in the 2nd-6th months of pregnancy. Women suffering from lumbosciatic pain during pregnancy can respond very well to this treatment method. However, our experience in this field is still quite limited: therefore, pregnant women should not undergo this kind of treatment.
1. What is the Active Lumbar Traction?
It is a physiotherapic method for the treatment of lumbar and sciatic pain.
2. Who can prescribe this treatment and who can apply it?
This treatment must be prescribed by a physician and administered by qualified therapists.
3. How is the treatment carried out?
The patient "pulls" himself/ herself while positioning arms and legs on a special treatment table. The table is horizontally divided into two parts, which are electrically operated by thetherapist. The patient exerts maximal active traction efforts for 5/6 seconds and then relaxes for 20/60 seconds. Between one traction and the other or during traction time, the spine ispositioned so as to make the patient's efforts painless. All spine movements are expected to become less painful or completely painless.
4. How long does a treatment cycle last?
The treatment begins with 3 outpatient sessions, each with a duration of half an hour, to be carried out every other day. If an objective improvement is obtained, the treatment will continuewith 3-6 additional sessions.
5. What are the differences between ALT and traditional traction?
ALT is a kind of active physiotherapy associated with a passive mobilization of the lumbosacral spine. Although their names are similar, ALT and the conventional passive tractions differ completely.
6. What are the differences between ALT and Natlhev's swedish autotraction method?
Although the ALT therapy is based on the principles of autotraction, the method has been:modified in a number of waysa) the treatment table has been considerably simplifiedb) the treatment technique is much easier: atherapist can learn it in just one day;c) the treatment can be applied to patients affected by a wider range of clinical symptoms.For example, patients who do not feel a change in pain intensity in relation to the different spine positions can be submitted to this treatment, whereas according to Lind-Natchev's autotraction method this had to be a preliminary condition.
7. Which patients are eligible for treatment?
Those affected by lumbar or sciatic pain of a mechanical origin, for example herniated discs, disc protrusions and narrow lumbar canal either congenital or acquired. The studies on effectiveness which have been published so far are mainly concerned with patients suffering from long lasting symptoms. Nevertheless, also patients who complain of a recently developed pain can respond to treatment very well. It is not advisable to treat patients while they are free from symptoms: the preventive effectiveness of the treatment against future attacks of lumbosciatic pain has not been proved yet.
8. Does AU work in the treatment of post-surgical syndromes, as well as relapsed herniations?
Yes, it does. Its effects are similar to those produced in patients who have not undergone surgical interventions.
9. What are the possible effects?
On the average, pain intensity can be reduced to even less than one third in 50-70% of the patients and very often it can disappear, too. The results are permanent. Very often the treatment produces a normalizing effect on the Lasepue sign and on possible strength deficits.
10. Is the patient expected to follow any particular precautions after treatment?
No aftercare is required. A general back-sparing lifestyle is advisable (for example it is better to avoid overweight or sudden spine extensions/ rotations, etc.).
11. Is it possible to administer the AU treatment together with other therapies?
Yes, it is. ALT can be applied together with any other pharmaceutical or physiotherapic treatment. This, however, can make it difficult to decide whether the possible improvement produced after the first three sessions is due to the ALT treatment alone or to other therapies.
12. Which is the relation between the treatment effects and the clinical picture of the candidate patient?
There is almost no relation. Patients affected by severe pain caused by multiple disc herniations can respond better than patients with light pain caused by an isolated disc protrusion.
13. Are there any contra-indications?
The physician prescribing the treatment has to decide for each single case whether there are contra-indications or not. As a rule, treatment is not recommended during pregnancy. Patients affected by abdominal herniations, prolapses or by serious varices can report a temporary worsening of their symptoms (traction efforts require a Valsalva manoeuvre). Osteoporosis requires caution during treatment because of the vertebral stress produced by the contraction of the paraspinal muscles.Obviously, the method has no effects on pain due to major spinal inflammations (e.g. ankylosing spondilitis) or neoplasms, which are to be considered as contra-indications. Possible cervical pain can intensify owing to certain manoeuvres but only during the session, not at a later time. In this case it is sufficient to move the patient's head to a more comfortable position, choose softer manoeuvres and make the treatment sessions less frequent. Treatment is not advisable in case of serious heart diseases.
14. Can the treatment lead to a symptomal worsening?
About 10% of the patients complain of an intensification of lumbar or sciatic pain for 2- 5 days after treatment. This does not compromise final success. It is only advisable to wait for pain to become less acute and then go ahead with the treatment cycle as planned.
15. How does the technique work?
Probably the adjustments of the treatment table produce favourable micro-alterations in the disk profile and/or a decongestion of the dural veins engorged because of compression and/or inflammatory reaction.

Introduction - The effects of spinal traction - Types of spinal traction - Continuous traction - Intermitent mechanical traction - Manual traction - Positional traction - Active Lumbar traction - Indications and contraindications - Herniated disc with protrusion - McKenzie’s extension basics - Degenerative discopathy - Articular hypomobility (Articular dysfunction) - Contraindications for spinal traction - Lumbar traction techniques - Introduction - Traction weights and body friction - A table with mobile sections - The patient must be in relax - Traction belts - Patient’s positions - Type of traction - Prone position - Protective scoliosis - Cervical traction techniques - Introduction - Traction angles - Chin strap - Traction weights - Patient in relax - Treatment duration - Temporomandibular joint - Manual cervical traction - Unilateral cervical traction - Conclusions
Brochure, Ed. July 2021, English. 56 pages.

